

For detection of measurable residual disease (MRD) in acute myeloid leukemia with NPM1 mutations, RT-qPCR with quantification of leukemic transcripts is currently considered the method of choice; however, MRD can also be determined with DNA-based methods, offering certain advantages. For example, digital droplet PCR (ddPCR) and targeted deep sequencing (deep seq) do neither require standard curves nor reference genes and are thus less labor intense than RT-qPCR. Also, deep seq allows for quantification independently of type of NPM1 mutation. In addition, DNA-based techniques enable MRD assessment of other mutations, beyond the reach of RT-qPCR, which is limited to analyses of highly expressed genes or fusion transcripts (e.g. core binding factor leukemias). With the rapid development of highly sensitive DNA-based techniques for MRD detection, there is a need to establish clinically relevant cut-offs for accurate interpretation of MRD results and risk stratification. Here, we compare and provide MRD cut-offs for three different DNA-based MRD methods for NPM1 mutations: quantitative PCR (qPCR), ddPCR and deep seq.
To compare the DNA-based methods with RT-qPCR, we analyzed 110 follow-up peripheral blood (PB) or bone marrow (BM) samples from 32 AML patients harboring NPM1 mutation type A. First, we compared the mere detectability of leukemic signals (without reference to specific MRD cut-off points). We found a high correlation between results from RT-qPCR and the three DNA-based methods (Rs=0.936 for RT-qPCR vs qPCR, Rs=0.774 for RT-qPCR vs ddPCR and Rs=0.743 for RT-qPCR vs deep seq, p<0.001). As expected, RT-qPCR was the most sensitive method. Among the DNA-based methods, qPCR was the most sensitive, detecting leukemic DNA in 95% (55/58) of the RT-qPCR positive samples, compared to 72% (42/58) and 62% (36/58) for ddPCR and deep seq, respectively. Interestingly, the transcript level for a given amount of measurable leukemic DNA (RNA copy number per leukemic DNA molecule) fluctuated considerably between different follow-up samples for certain patients. In some cases, the RNA/DNA ratio exceeded a hundredfold difference between different follow-up time points in both PB and BM. Hence, transcript analysis may be more complex than just a simple measurement of leukemic cell burden, which in turn may influence accurate risk stratification and treatment decisions, if relying on RT-qPCR measurements alone.
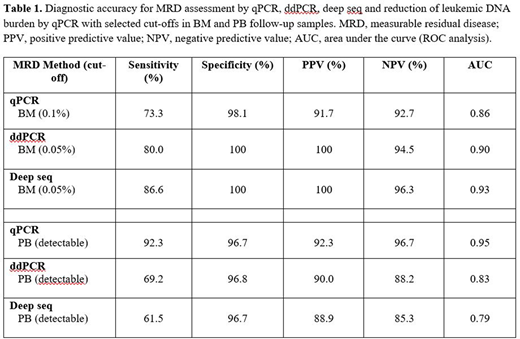
To select adequate DNA MRD cut-offs, we performed ROC curve analyses for each method at various DNA cut-offs, comparing them with the gold standard RT-qPCR cut-off. In BM, this cut-off can be defined as a less than 3 log reduction of mutated NPM1 transcripts vs diagnosis, separating MRDhigh from MRDlow/undetectable (sometimes inaccurately termed "MRD-positivity" and "MRD-negativity", respectively). In PB, the mere detectability of mutated NPM1 transcripts is considered the relevant cut-off. DNA cut-offs were chosen based on the area under the curve (AUC) for the ROC analyses (Table 1), and influenced by available literature including recommendations of prognostically relevant MRD levels. For qPCR, a cut-off at 0.1% leukemic DNA was judged relevant in BM. For ddPCR and deep seq, 0.05% was chosen to adjust for measuring allelic ratio (variant allele frequency (VAF)) rather than mutant DNA alone. In PB, the selected cut-off was detectable leukemic signal irrespective of DNA method.
We next determined the accuracy of the selected cut-offs, for identification of samples with clinically relevant MRD, by comparing them with the gold standard RT-qPCR. In general, the selected DNA cut-off values generated high specificity as well as high positive and negative predictive values (Table 1). The vast majority of all MRD analyses (93% (368/395)) showed concordant results irrespective of MRD method. In BM samples, MRD assessment by the DNA based methods agreed with MRD status as determined by RT-qPCR (MRDhigh high vs MRDlow/undetectable) in 93% (62/67) of the analyses for qPCR, 96% (64/67) for ddPCR, and 97% (65/67) for deep seq. In PB, the agreement was 95% (41/43), 88% (38/43) and 86% (37/43), respectively.
In summary, we found strong agreement between different MRD methods and based on this could provide clinically relevant cut-offs for risk stratification. Thus, in BM follow-up samples from AML patients with NPM1 mutation, we propose 0.1% leukemic DNA as cut-off for qPCR and 0.05% VAF for ddPCR and deep seq.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal